
When non-surgical treatments fail to treat osteoarthritis of the knee, surgery may be the best next step.
Now, there are several surgical techniques for this type of knee arthritis. The best for you will depend on your age, symptoms, lifestyle, and other factors.
Your surgeon will know best which surgery will benefit you the most. But, you can use this guide to help you set realistic expectations on their outcomes.
This is what we’ll cover. Tap on any of the topics to go to their sections:
- Knee arthroscopy (lavage, debridement, meniscectomy)
- Cartilage repair procedures (bone marrow, OATS, ACI)
- Tibial osteotomy procedure
- Knee replacement surgery (partial and total)
- Risks associated with knee osteoarthritis surgery
- How to know if you need surgery for your knee arthritis?
- FAQs
Knee arthroscopy for osteoarthritis

In arthroscopic surgery, the orthopaedic surgeon operates with tiny instruments and a camera. This causes less trauma to the joint, which often means a faster recovery.
Now, this procedure won’t stop the progression of osteoarthritis – no surgery can. But for well-selected patients, it can repair some of the joint damage, thus causing less pain. (1)
On average, the recovery period is between 2 to 6 weeks. You’ll likely feel joint pain, swelling, and stiffness during the first days while you heal. (2)
Learn more: Our complete guide on knee osteoarthritis – from causes to best treatments
For knee osteoarthritis, there are two main arthroscopic techniques your surgeon can perform:
1) Knee joint lavage/debridement
Here, the goal is to remove or smoothen the damaged joint surfaces that could be locking your knee or causing pain. This can be done in two ways (3):
- Lavage: The surgeon “washes out” the joint surface with saline solution to remove cartilage fragments.
- Debridement: The surgeon smoothens the joint with surgical instruments.
These procedures make sense – on paper. Research shows they give similar results to physical therapy and medication, but with more side effects. (3)

And interestingly, doing lavage/debridement for knee OA often provides the same results as sham surgery. (4)
That’s why the AAOS doesn’t recommend performing these techniques. At least, not for knee osteoarthritis – the risks outweigh the benefits. (4)
Yet, lavage could provide pain relief in knee osteoarthritis if it’s due to intra-articular crystals. (4) And, people with bone necrosis may benefit the most from debridement. (1)
2) Knee joint meniscectomy
In this other arthroscopic technique, the surgeon removes a part or all the damaged meniscus.
Nowadays, the goal is to keep as much of the meniscus as possible to avoid future knee joint issues. So, partial meniscectomy should be preferred over a total one, according to studies.
And, according to the AAOS, a partial meniscectomy can be used in knee osteoarthritis in people with (4):
…mild-to-moderate knee OA and an MRI confirmed meniscal tear who have previously failed appropriate conservative treatment such as physical therapy, corticosteroid injections, and a course of non-steroidal anti-inflammatory medications. – AAOS guidelines, 2021
Otherwise, this surgery could provide the same results as physical therapy, but with more risks and side effects. (3, 4)
Procedures for repairing cartilage damage
Articular cartilage is really hard to heal on its own. But, certain procedures can help it recover, if the area of damaged cartilage is small.
The downside is that very few people may benefit from these procedures. For them to work, the patient must meet these conditions (1):
- Be young.
- No knee deformity.
- No patella tracking issues.
- Have healthy ligaments.
Now, the most common procedures for healing knee cartilage are (1):
Bone marrow stimulation
Through arthroscopy, the surgeon makes small but precise fractures on the bone. This stimulates the growth of healthy cartilage. A similar result can be achieved with abrasion or drilling instead of fracturing.
But, there’s no way to know how much joint cartilage will grow, if any.
Osteochondral transplantation techniques
Also known as “mosaicplasty,” this procedure consists of transplanting articular cartilage from one site – often the femur – to another.
This procedure can be done through open surgery or arthroscopy. This will depend on the size of the damaged cartilage area.
Autologous chondrocyte implantation (ACI)
This procedure consists of harvesting part of your cartilage and growing it in a lab for 3-4 weeks. Then, the surgeon implants this new cartilage into the injured area.
However, it’s a fairly long and expensive procedure.
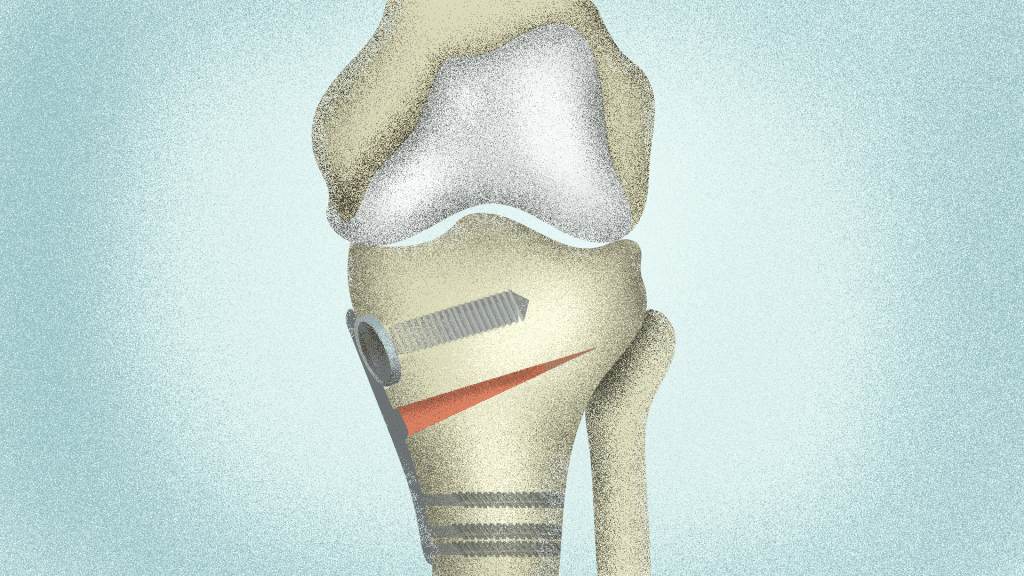
Knee osteotomy
This surgical procedure might relieve pain from wear and tear arthritis if these conditions are met (1, 4):
- The patient is <60 years old,
- Has knock-knees or bowlegs, and
- A confirmed unicompartmental knee osteoarthritis (wear and tear in one side of the joint).
In an osteotomy, the surgeon cuts a wedge from the shin bone or the thigh bone to improve the alignment of the knee. Then, uses screws, plates, or other hardware to keep the wedge open or closed. (1)
This redistributes the load on the joint, decreasing the pressure on the affected side and reducing pain. (1)
The best thing about an osteotomy is that it can delay the need for knee replacement surgery.
Most patients feel satisfied with their osteotomies after 2 years, but this tends to decrease over time. At the 9-year mark, +60% of the patients may not feel satisfied with it and could need a replacement. (1)
That’s why this procedure is mostly recommended for active and younger people. It won’t repair the cartilage damage, but it buys it more time.
Now, if you have unicompartmental osteoarthritis and are close to 50-60 years old, a better option could be a partial replacement. (1)
Knee joint replacement surgery
This procedure is also known as “knee arthroplasty.” Here, the orthopedic surgeon will replace a part or the totality of the knee with an artificial joint – a knee prosthesis.
Replacing the joint is an irreversible procedure, and a prosthesis tends to last between 10 to 20 years. That’s why a knee replacement is recommended for patients that (1, 3):
- Have tried rehabilitation, medications, exercise, and other treatments without result.
- Have advanced knee OA.
- Are >60 years old.
- Their quality of life is severely affected due to their knee OA.
There are two types of knee replacement surgery:
Partial knee replacement surgery
This one is also known as “unicompartmental knee replacement surgery.” It can relieve knee pain and restore function in people with osteoarthritis in just one side of the knee joint.
But for this surgery to be successful, the cartilage and meniscus on the other side of the knee must be healthy. The cruciate ligaments should be well-preserved as well. (1)
The prosthesis can last up to 10 years. This is true for 80 to 98% of people undergoing partial knee replacement surgery. (1)
Total knee replacement surgery
Here, the surgeon replaces all the joint with a new knee. It’s the best treatment for people with severe knee OA, after the other treatment options have failed. (1, 3)
A crucial factor here is making sure you need a total knee replacement, though. This is because according to research (1, 3):
- Up to 25% of people that underwent knee replacement surgery didn’t need it, which made their symptoms worse.
- 1 out of 8 patients still have knee pain and disability, despite their X-rays don’t show abnormalities.
To not count yourself into these statistics, please go to a physical therapist to treat your knee pain first. Follow theirs and your doctor’s recommendations before and after surgery, too.
This may help: Knee replacement pain at night – when to worry?
Risks of surgical treatment for knee arthritis
Generally, the more invasive the surgery, the more risks of complications. They include, but aren’t limited to (3, 4, 5):
- Infection – on the wound and/or deep in the joint.
- Worsening of knee pain.
- Blood clots.
- Premature joint replacement.
- Pulmonary embolism.
- Nerve damage in and/or around the surgical site.
- Injury of the ligaments.
- Leg length discrepancy.
- Knee dislocation.
- Fracture.
- Reoperation.
For knee replacement surgery, whether partial or total, there’s a risk of breaking or loosening the implant. And although very rare, there’s a risk of death – but this is true with any surgery.
When is surgery necessary for osteoarthritis of the knee?
Here are some instances when surgery is necessary for knee OA, such as:
- Physical therapy and medications can’t relieve pain anymore.
- No home treatment for knee OA eases your symptoms.
- Your quality of life has severely deteriorated due to this condition.
However, we know these factors are highly subjective. That’s why we made a guide to help you know whether you need surgery for knee OA or there are some things you can try.
Further reading: 15 evidence-based treatments ranked from best to worst.
FAQs
Can knee osteoarthritis in the knee be fixed by surgery?
Yes. But only if non-surgical treatments such as physical therapy, injections, medication, or weight loss have failed.
What is the best surgery for knee osteoarthritis?
The best surgery will depend on your specific symptoms, age, lifestyle, medical history. Your surgeon will recommend the best surgical technique for you.
How long does it take to recover from arthritis knee surgery?
The recovery time is anywhere from a few weeks to months. This depends on several factors, such as the type of surgery, your medical history, or your adherence to physical therapy.
Conclusion: Surgery for osteoarthritis of the knee pain
Any knee surgery comes with serious potential side effects. So, please make sure to do your conservative treatment before going under the knife.
However, if your doctor and physical therapist suggest knee surgery, there are excellent hip and knee surgeons out there. Use this guide to help you make an informed decision.
Resources
- Rönn, Karolin et al. “Current surgical treatment of knee osteoarthritis.” Arthritis vol. 2011 (2011): 454873. DOI: 10.1155/2011/454873
- Siemieniuk, Reed A. C. et al. “Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline.” British journal of sports medicine vol. 52,5 (2018): 313. DOI: 10.1136/bjsports-2017-j1982rep
- The Royal Australian College of General Practitioners. Guideline for the management of knee and hip osteoarthritis. 2nd edn. East Melbourne, Vic: RACGP, 2018. Retrieved on February 2022 from: https://www.racgp.org.au/download/Documents/Guidelines/Musculoskeletal/guideline-for-the-management-of-knee-and-hip-oa-2nd-edition.pdf
- American Academy of Orthopaedic Surgeons Management of Osteoarthritis of the Knee (Non-Arthroplasty) Evidence-Based Clinical Practice Guideline (3rd Edition). https://www.aaos.org/oak3cpg Published August 31, 2021.
- Healy, William L et al. “Complications of total knee arthroplasty: standardized list and definitions of the Knee Society.” Clinical orthopaedics and related research vol. 471,1 (2013): 215-20. DOI: 10.1007/s11999-012-2489-y


